Starting, 1 July, millions of Medicare enrollees will gain coverage for weight-loss drugs for the first time, through a temporary pilot programme called the Medicare GLP-1 Bridge. The scheme covers Zepbound, Foundayo and Wegovy at a $50 monthly copayment and marks the first time Medicare has helped pay for drugs prescribed solely for obesity, rather than for diabetes or cardiovascular conditions. The health policy research organisation KFF estimates that roughly 3.8 million beneficiaries could be eligible.
That figure represents roughly 8 percent of the 47.5 million people enrolled in Medicare Part D, the prescription drug benefit through which the Bridge will operate, even though the programme itself sits outside the standard Part D payment structure.
How the programme works
The Medicare GLP-1 Bridge is a short-term demonstration run by the Centers for Medicare and Medicaid Services (CMS) under its authority to test new payment and coverage models. It will run from 1 July 2026 through 31 December 2027. Because Medicare is prohibited by statute from covering weight-loss drugs outright, CMS has used Section 402(a)(1)(A) of the Social Security Amendments of 1967 to create the time-limited scheme rather than changing the underlying law.
“Medicare is not changing the law right now,” said Juliette Cubanski, Vice President and Director of Medicare policy at KFF. “What it’s doing is taking advantage of a specific section of the law that gives the federal government the ability to stand up a temporary programme.”
Eligible beneficiaries enrolled in a participating Part D plan, whether a standalone prescription drug plan or a Medicare Advantage plan with drug coverage, will pay a flat $50 copayment for a 30 day supply. Crucially, this payment will not count towards the Part D deductible or the annual out-of-pocket spending cap, and the Part D Low-Income Subsidy, known as Extra Help, cannot be applied to reduce it. Manufacturers have agreed to supply the eligible drugs to the programme at a net price of approximately $245 per monthly prescription, with CMS using a single central processor to manage prior authorisation, claims adjudication and payment to pharmacies rather than routing claims through individual Part D plans.
Who qualifies for the Medicare GLP-1 Bridge
Eligibility is built around body mass index (BMI) thresholds combined with specific clinical conditions, mirroring criteria used in FDA labelling for these drugs. According to CMS guidance, a beneficiary qualifies if they have a BMI of 35 or higher with no further condition required, a BMI of 30 or higher together with heart failure with preserved ejection fraction, uncontrolled hypertension, or chronic kidney disease at stage 3a or above, or a BMI of 27 or higher together with prediabetes, a previous heart attack or stroke, or symptomatic peripheral artery disease.
These criteria must be met at the point a beneficiary first started GLP-1 therapy, even if that predates the launch of the Bridge programme. CMS has indicated that a patient who began treatment with a qualifying BMI but has since lost weight will not be excluded, provided their prescriber attests that the original threshold was met at initiation.
A number of exclusions apply. Beneficiaries are not eligible if they already receive a GLP-1 medication through their regular Part D drug plan for an approved indication such as type 2 diabetes, or if they have a diagnosis of moderate to severe obstructive sleep apnoea or metabolic dysfunction associated steatohepatitis (MASH), often referred to as fatty liver disease. KFF’s analysis found that while 9.7 million Part D enrollees met the underlying clinical criteria in 2023, fewer than half, the estimated 3.8 million, would actually qualify once these exclusions and existing GLP-1 prescriptions were taken into account.
The drugs covered
Three medications will be available under the Bridge: Novo Nordisk’s Wegovy, available as both an injection and an oral tablet, Eli Lilly’s Zepbound in its KwikPen injectable formulation, and Eli Lilly’s newer oral pill Foundayo, the brand name for orforglipron. Single-dose Zepbound vials and pens are explicitly excluded from coverage, meaning prescriptions must specify the KwikPen format.
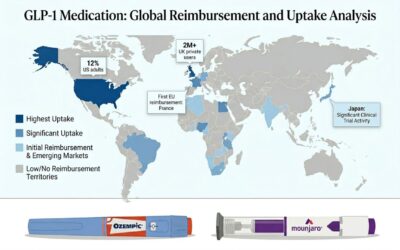
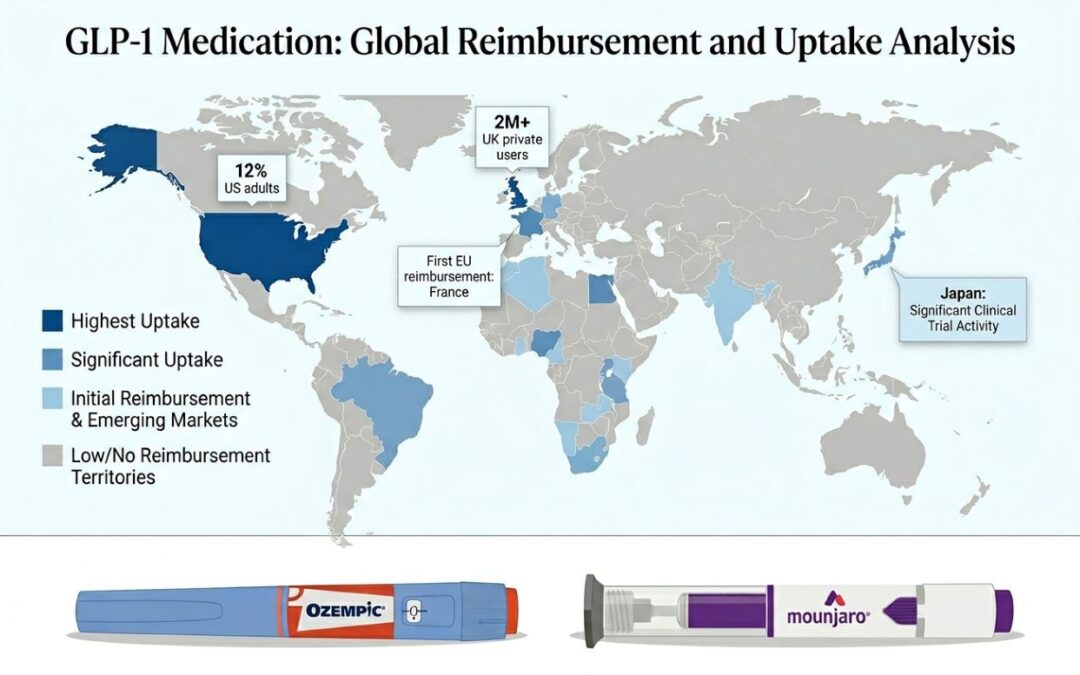
Foundayo, approved by the FDA on 1 April 2026, is a small-molecule, non-peptide GLP-1 receptor agonist that can be taken at any time of day without the food and water restrictions that apply to oral semaglutide. In Eli Lilly’s Phase 3 ATTAIN-1 trial, participants taking the highest dose who remained on treatment lost an average of 27.3 pounds, or 12.4 percent of body weight, over 72 weeks, compared with 2.2 pounds in the placebo group. Deborah Horn, director of the Center for Obesity Medicine at McGovern Medical School at UTHealth Houston, said the drug offers patients who cannot or do not wish to take an injectable medication greater flexibility in how they approach their treatment. The pace of GLP-1 adoption is not unique to the United States; our earlier coverage examined how GLP-1 uptake is booming across global markets, from the United States to France and beyond.
The human impact
For many beneficiaries, the programme represents a long-awaited reduction in cost. Cash prices for these drugs without insurance typically run between $149 and $449 a month depending on the medication and dose, figures that have placed them out of reach for many older adults on fixed incomes. Catherine Varney, Obesity Medicine Director at the University of Virginia and a trustee of the Obesity Medicine Association, said many of her Medicare patients have serious cardiac risk factors that make access to treatment urgent.
“Most of these patients that I wanted to start on this medication are ticking time bombs,” Varney said. “They’ve got prediabetes, high blood pressure, high cholesterol, all these cardiac risk factors that are leading to heart attack and stroke.”
Even at $50 a month, however, Cubanski cautioned that the copayment could remain unaffordable for some lower-income beneficiaries, particularly because Extra Help subsidies cannot be used to offset it. KFF has separately noted that this creates an access barrier precisely among the population for whom affordability is most constrained, a point also raised in CBS News reporting on the programme’s launch.
Cost to the federal government and what comes next
CMS has not published its own cost or enrolment projections for the Bridge programme, but KFF estimates that if between 10 and 25 percent of the 3.8 million eligible beneficiaries enrol and fill a monthly prescription through the end of 2027, the programme could cost Medicare between $1.3 billion and $3.3 billion, based on 2023 data. That estimate does not account for any offsetting savings from improved beneficiary health outcomes.
The Bridge was originally intended as a precursor to a longer-term coverage framework called the BALANCE Model, short for Better Approaches to Lifestyle and Nutrition for Comprehensive hEalth, which had been scheduled to begin for Medicare Part D in January 2027. In April 2026, however, CMS announced it would delay the Part D component of BALANCE indefinitely and instead extend the Medicare GLP-1 Bridge through the end of 2027, giving the agency more time to collect data on GLP-1 utilisation before any permanent policy decision.
What happens after the Bridge expires at the end of 2027 remains uncertain. Without a further extension from CMS or a change in the underlying law by Congress, beneficiaries could lose Medicare coverage for GLP-1s prescribed solely for weight loss.
“In the short term, we have this temporary programme, and then no clear path forward yet as to what will happen at the end of 2027,” Cubanski said.
Beneficiaries who believe they may be eligible are advised to speak with their prescribing clinician, who can help determine whether they meet the BMI and clinical criteria and submit the necessary prior authorisation request through the central processor once the Medicare GLP-1 Bridge opens on 1 July.