In the medical field, being “authorized” and “qualified” are two very different things. Authorized generally indicates you have the legal right to practice. Qualified means you have the expertise, experience, and skill needed to practice effectively.
The distinction between the two designations has become very clear in the world of peptide medicine. The authorized pool in peptide medicine includes essentially any licensed prescriber in the country. In most states, MDs, DOs, NPs, and PAs can legally write prescriptions for peptides being compounded under an appropriate legal framework. That’s millions of clinicians.
The qualified pool, meaning prescribers with formal training in evidence-based peptide pharmacology, dosing, contraindications, monitoring, and adverse event recognition, is a fraction of the authorized pool. And because there’s no specialty board, no required continuing medical education, no standardized curriculum, and no credentialing requirement specific to peptide medicine, distinguishing between the two is challenging.
But opting for qualified over authorized is critical to avoiding serious health risks. Prescribers who lack experience and expertise may make missteps, such as:
- Using outdated or incorrect dosing protocols copied from supplier marketing materials or social media sources.
- Putting patients on inappropriate combinations due to a lack of understanding of how compounds interact.
- Missing contraindications, particularly around thyroid history, malignancy history, and certain cardiovascular conditions.
- Providing inadequate monitoring during use.
- Misattributing adverse events that are peptide-related.
Why is there a gap in peptide medicine between authorized and qualified prescribers?
The gap between authorized and qualified emerged in peptide medicine due to timing. Peptide medicine grew commercially before it grew institutionally.
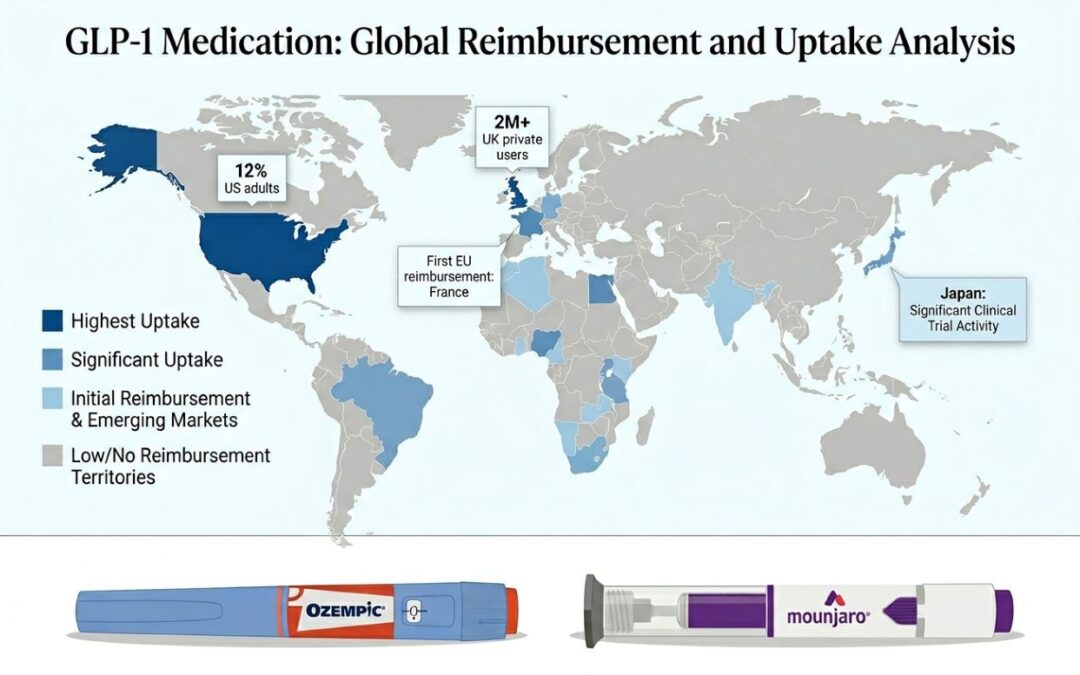
Clinical research on peptides has been advancing for decades, but the explosion in consumer demand occurred over roughly the last five years, driven by GLP-1s on one side and the wellness and longevity movement on the other. Medical schools don’t teach peptide pharmacology in any depth, and specialty boards haven’t moved on it.
The peptide field expanded faster than the credentialing systems that would normally govern it. And until credentialing catches up, practitioners and patients need to know where the dangers lie and how to avoid them.
What key factors qualify someone to prescribe peptides?
There are a number of factors that qualify someone to prescribe peptides, but any one of them alone is not enough.
One critical qualifier is formal pharmacology training in the peptide class. A weekend course or webinar series funded by a supplier is not sufficient. Being qualified involves participating in genuine education on how peptides work, what the evidence base looks like, where the evidence is solid or where it’s still emerging, and the limits of peptide science. A qualified prescriber should be able to articulate what they don’t know about a given peptide, not just what they’ve been told.
A working understanding of the regulatory landscape is another key qualification. Those prescribing peptides should know which ones are FDA-approved for which indications, which are being compounded under what legal framework, and the differences between a 503A pharmacy, a 503B outsourcing facility, a research peptide vendor, and the grey market.
Prescribers who don’t understand the legal context of what they’re prescribing are risking exposure to enforcement actions. Those prescribers are also usually working with sources that aren’t defensible.
One of the most important qualifiers in today’s peptide market is the willingness to say no to a patient who wants a prescription that isn’t appropriate for their situation. That sounds basic, but it isn’t the norm in the “Wild West” landscape of peptide medicine. In a market where patient demand is driving most prescribing, the discipline to push back matters more than the discipline to prescribe.
Why is it critical to close the credentialing gap in peptide medicine?
Without credentialing, the field of peptide medicine will continue growing commercially while the quality gap widens. Without shifting the space away from authorized and toward qualified, there will be more prescribers entering without training, more patients receiving suboptimal or actively harmful care, more adverse events going unrecorded, and eventually a high-profile patient-harm event that catalyzes a regulatory crackdown.
It’s important to note that an FDA enforcement against compounding pharmacies or a state medical board action against prescribers won’t distinguish between legitimate clinicians who do this well and those who shouldn’t be in the space. Everyone gets caught in the same net.
To see what a crackdown would look like, look at the history of adjacent therapeutic categories such as stem cell clinics in the late 2010s or ketamine clinics more recently. As commercial growth outpaces institutional infrastructure, harm accumulates, regulators step in with a heavy hand, and the legitimate operators end up paying for the bad actors.
While the industry waits for regulators to catch up, establishing a private trust infrastructure can remedy many of the problems in peptide medicine by putting credentialing in place for prescribers that defines what “qualified” actually means and verifies it. It recognizes pharmacies that meet defensible quality standards so prescribers and patients can identify them. It provides research authorization for sites that generate real-world evidence, so the evidence base catches up with commercial reality.
None of this replaces the FDA or state medical boards. It supplements them in the space those bodies were never designed to occupy.
When that infrastructure works, the field professionalizes from within rather than getting professionalized from above. Clinicians have a credible signal of who’s qualified. Patients have a way to identify safe sources. And regulatory action, when it does come, can be more surgical because the legitimate operators have already differentiated themselves.
Peptide medicine is inching away from a “Wild West” atmosphere on the margins of the wellness movement and toward mainstream clinical practice. But it still lacks the order and accountability needed to ensure that the prescriptions patients receive are medical rather than merely transactional.
The prescribers who establish themselves as legitimate clinicians in this category now will have a meaningful head start when insurance starts covering it, hospital systems start incorporating it, and the patient population shifts from early adopters to mainstream chronic disease management. Those who treat credentialing as a cost will find themselves outpositioned by those who treat it as an investment.
Author Bio

Karthik Achari is the Founder and Clinician of PepMD, the first private accreditation and credentialing body purpose-built for peptide medicine. A clinician by training, Achari attended Bradley University’s Doctor of Nursing Practice/Family Nurse Practitioner program and built his perspective on healthcare by working with providers to optimize peptide prescribing practices and by operating healthcare businesses. This dual experience has given him a comprehensive understanding of how the system functions in practice, where standards exist, where they fall short, and where critical gaps remain. In 2026, Achari founded PepMD to address the rapid growth of peptide medicine without the infrastructure needed to support it. Modeled in part after established accreditation systems like The Joint Commission, PepMD credentials clinicians, recognizes pharmacies, and authorizes research sites under a single, unified standard. Achari also founded Pure Rx, a pharmaceutical infrastructure company, where he identified firsthand the need for greater accountability and consistency in the peptide and GLP-1 landscape. His work focuses on bringing structure, credibility, and oversight to an evolving sector that has outpaced traditional regulatory frameworks.